Ivanusic laboratory: Pain and sensory mechanisms
Research Overview
Our ability to sense and react to our environment is governed by activity in sensory neurons. Small diameter peripheral sensory neurons can detect tissue damage (generating pain), local changes in temperature and mechanical stimuli. A more complete understanding of the mechanisms by which these stimuli generate nerve impulses in peripheral sensory neurons, and how these are altered in conditions (such as inflammation) that heighten pain, thermal and mechanical sensitivity, will allow us to better define ways in which we can treat pain.
NEURAL MECHANISMS OF SKELETAL PAIN
Pain associated with skeletal pathology or disease puts a significant burden (both in terms of quality of life and cost) on individuals, society, and the health care systems worldwide. Pain is the major reason why most of these patients present to the clinical environment. Opioids and non-steroidal anti-inflammatory drugs (NSAIDs) are used to treat mild to severe bone pain, but therapeutic use over long periods required to treat chronic or intractable bone pain is limited by severe and undesirable side-effects. There is a clear need to identify alternative approaches for the management of skeletal pain.
Major impediments to the development of alternative strategies to treat bone pain is the significant challenge of experimental access to nociceptors in bony tissue. Our lab has developed and routinely uses a number of different approaches to study how bone nociceptors transduce and code information about noxious stimuli applied to bone, and how this is altered in skeletal pathology or disease. We also use these approaches to assay the effects of potential therapeutics. This is critical to the development of more targeted and specific therapies to treat bone pain.
Our aim is to explore how peripheral sensory neurons that innervate bone contribute to the experience of skeletal pain, and how their function is affected by skeletal pathology and disease.
We have already shown that the periosteal, medullary and trabecular compartments of bone are all innervated by sensory neurons that are responsive to noxious chemical, mechanical and/or inflammatory stimuli, and have neurochemical phenotypes consistent with a role in nociception. We have been among the first to document activity in the central nervous system related to stimulation of nerves in bone, and have developed animal models of inflammatory bone and joint pain that have been used to test whether peripheral application of specific drugs may be of use in the treatment of inflammatory bone pain. We have recently developed a highly novel in vivo electrophysiological bone-nerve preparation that allows us to record directly the physiology of bone nociceptors, and are currently the only group in the world that has the capacity to do this. We have also developed approaches to explore the neuroanatomical distribution of different types of sensory and sympathetic nerves in bone. We are currently using these approaches to study mechanisms that generate and maintain osteoarthritis pain, with a view to developing ways to treat it.
See references:
Nencini, S., Ringuet, M., Kim, D. H., Greenhill, C., and Ivanusic, J. J. (2018). GDNF, Neurturin, and Artemin Activate and Sensitize Bone Afferent Neurons and Contribute to Inflammatory Bone Pain. J Neurosci, 38(21):4899-4911.
Morgan, M., Thai, J., Nazemian, V., Song, R., and Ivanusic, J. J. (2022). Changes to the Activity and Sensitivity of Nerves Innervating Subchondral Bone Contribute to Pain in Late-Stage Osteoarthritis. Pain, 163(2): 390-402.
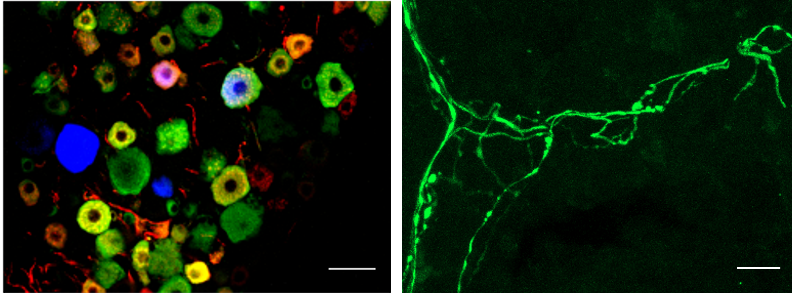
Figure 1: Immuno-labelling and light-sheet imaging of sensory neurons that innervate bone

Figure 2: Behavioural testing using weight distribution as a surrogate marker for pain
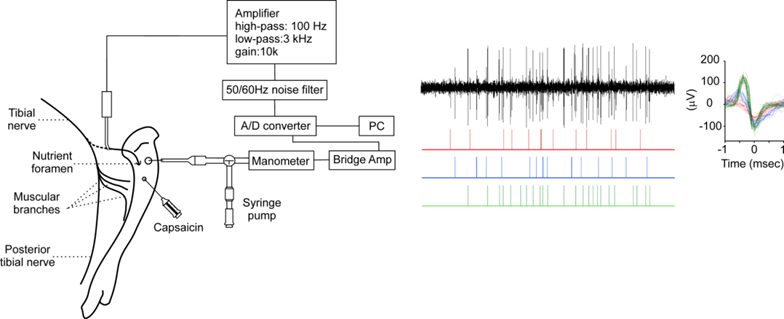
Figure 3: Schematic representation of the in vivo bone-nerve preparation and representative electrophysiological recordings
STRUCTURE/FUNCTION RELATIONSHIPS IN SENSORY NERVE TERMINALS OF THE CORNEA
Small diameter nerve terminal endings are responsible for transducing information about noxious and/or thermal stimuli applied to peripheral tissues. We are able to record directly from single small diameter sensory nerve terminals in the corneal epithelium. We use this technique to record electrical activity from single pain and cold-sensing nerve terminals in the guinea pig cornea and then, after marking the recording site, use immunohistochemistry and high resolution microscopy to determine the structure and neurochemical profile of the nerve terminals we recorded from. We have shown that functionally defined nerve terminals in the cornea can be distinguished on the basis of their morphology and neurochemistry, and that the morphology of endings can change in pathology, for example in diabetes. Our aim is to further explore how the morphology and neurochemistry of sensory nerve terminals influences their function in both health and disease (Collaborator: James Brock, University of Melbourne).
See reference:
Alamri, A., Wood, R. J., Ivanusic, J. J., and Brock, J. (2018). The Neurochemistry and Morphology of Functionally Identified Corneal Polymodal Nociceptors and Cold Thermoreceptors. PLOS ONE, 13(3):e0195108.
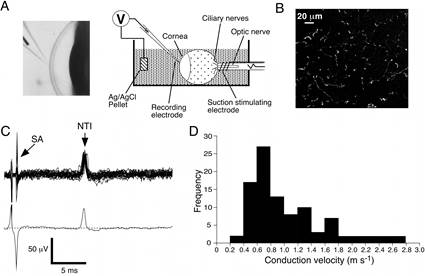
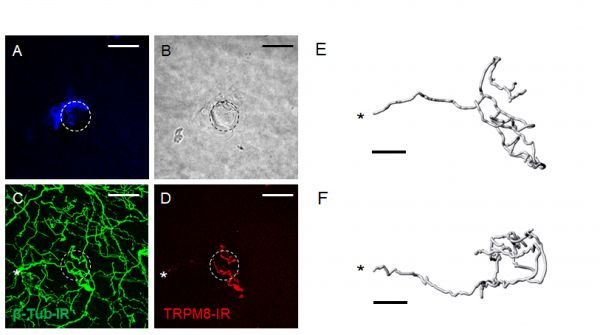
Figure 4: Morphological and molecular phenotyping of physiologically identified corneal sensory neurons and their nerve terminal endings
PAIN MANAGEMENT USING ULTRASOUND-GUIDED PERIPHERAL ANAESTHESIA
We have established a model in which we simulate ultrasound guided nerve blocks by injecting dye into human cadaveric material under ultrasound guidance, and then explore the extent of dye spread and nerve involvement, to provide an evidence base for the use of these nerve blocks in the clinical setting. We have published explorations of sciatic nerve, transversus abdominis plane, subcostal, thoracic paravertebral, fascia iliaca and erector spinae block, and most of these studies have directly informed clinical practice in anaesthesia. (Collaborator: Michael Barrington, St. Vincent’s Hospital, Melbourne)
See reference:
Cowie, B., McGlade, D., Ivanusic, J., and Barrington, M. J. (2010). Ultrasound-Guided Thoracic Paravertebral Blockade: A Cadaveric Study. Anesth Analg, 110(6):1735-9.
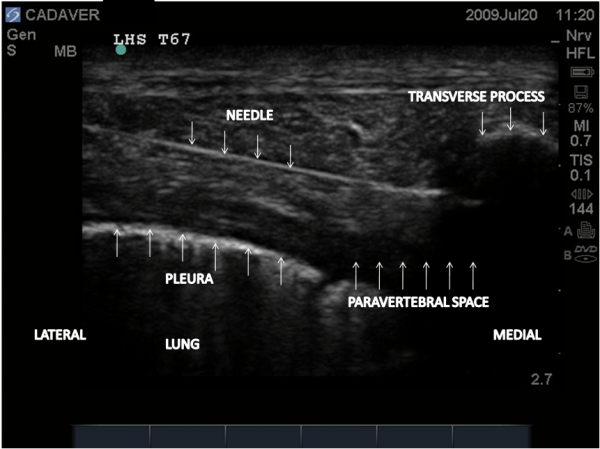
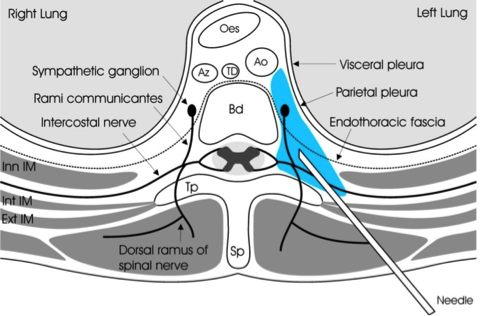
Figure 5: Ultrasound guided paravertebral block
Staff
Professor Jason Ivanusic
Associate Professor James Brock
Dr Michael Morgan, Research Fellow
Jenny Thai, Research Support Officer
Students
Vida Nazemian, PhD Student
Gao Xiong, PhD Student
Collaborators
Associate Professor James Brock
Professor Michael Barrington
Professor Stuart Mazzone